Introduction
Intestinal obstruction is the most common surgical emergency in the neonatal period.[1] Majority of intestinal obstructions in neonates have dynamic causes and their surgical management is straightforward.[2] However, there are some adynamic causes of neonatal intestinal obstruction which are rare, like congenital segmental intestinal dilatation (CSID) of small intestine and congenital enteric neuropathy.
Congenital segmental intestinal dilatation is a neonatal condition with unclear etiology and pathogenesis. Typically, the newborn with CSID presents with a limited (confined) bowel dilatation, usually ileum,and features of intestinal obstruction within days of birth.[2] The immature enteric ganglion cells, one of the forms of intestinal neuronal malformation, were reportedly observed in pre-term neonates and sometimes in term neonates with neonatal functional intestinal obstruction and Hirschsprung disease.[3] Immature ganglion cells in colon or rectum of neonates was thought to indicate transient functional immaturity of the intestine.[4] Pre-operative diagnosis is difficult because of the clinical polymorphism and the lack of specificity of radiological investigations.[5]
Around 150 cases of CSID has been published worldwide and this is the first case reportfrom Nepal. CSID associated with immature ganglion cells in colon has not been published so far, to the best of authors’ knowledge. We aim to describe this rare case which did not have typical characteristics of CSID and may be labelled as congenital segmental intestinal pseudo-dilatation (CSIPD).
Case Report
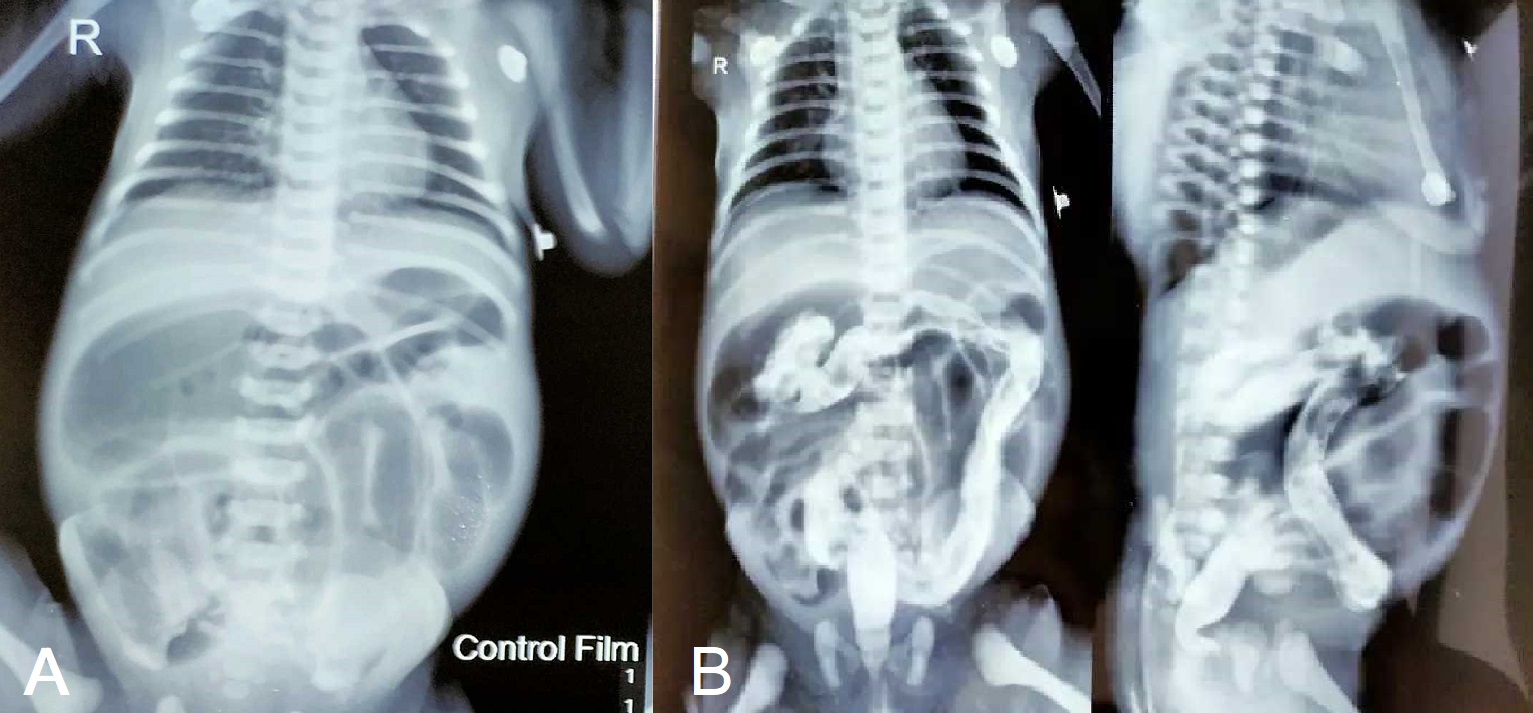
A full-term,3-day-old male baby presented with failure to pass meconium since birth, along with abdominal distension and bilious vomiting. Antenatal period was uneventful and he wasdelivered normally. At the time of admission, patient had features of some dehydration. Vital signs were stable. Abdominal examination revealed tense, distended abdomen with exaggerated bowel soundsand no palpable lump. Hernial orifices were intact. Perineal examination revealed normal positioned anal opening and well-formed external genitalia. After rectal stimulation, patient passed scanty amount of meconium. His biochemical parameters were within normal range except for mild hyponatremia (Hb: 16.9 g/dl; Platelets: 200,000 /cumm; WBC: 8,200 /cumm; Creatinine: 0.7; Sodium: 132 mmol/L; Potassium: 4.5 mmol/L, Total Bilirubin: 1.8 mg/dl; CRP: 12mg/L). Ultrasound of whole abdomen revealed normal scan. Water soluble contrast enema revealed normal looking colon with dilated small bowels suggesting small bowel obstruction (Fig. 1).
After optimizing general condition of the baby, exploratory laparotomy was performed which revealed a huge segmental dilatation (almost 4-5 times the size of normal) involving distal 6 cm of jejunum (Fig. 2). Distal to the jejunal dilatation, entire ileum was mildly dilated uniformly up to 10 cm proximal to ileocecal valve. There was no malrotation, intestinal atresia, volvulus, external bands, internal hernia etc. Milking of intestinal contents were done in both antegrade and retrograde manner to check patency of the bowel and for any web.Total colonic aganglionosis or other enteric neuropathies were suspected, and full thickness biopsies were taken from different parts of the colon (recto-sigmoid junction and transverse colon) including appendix. No intervention was performed on the dilated jejunal segment presuming it would resolve spontaneously as there was no abrupt transition to ileum which is unusual for a CSID.
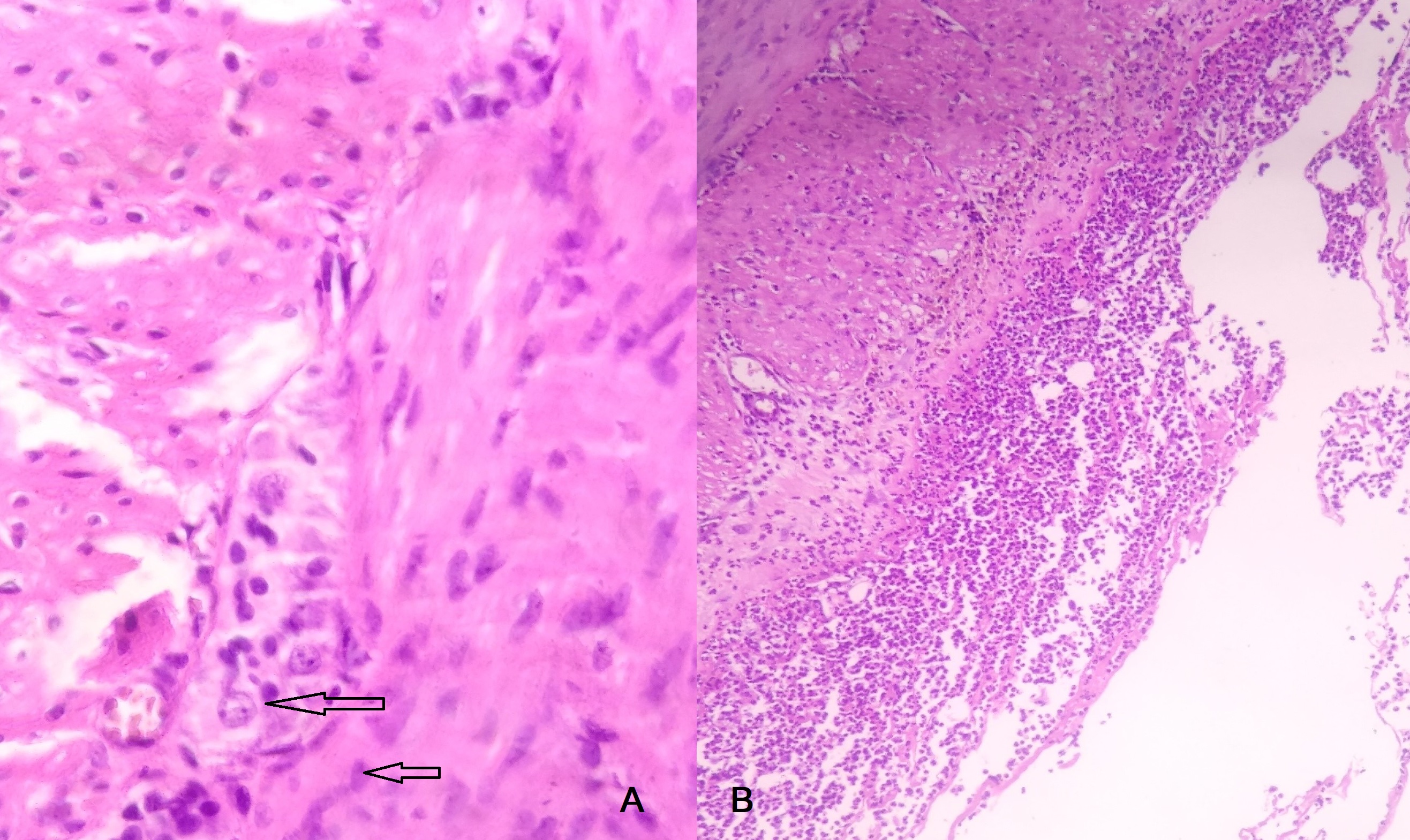
Post-operatively, abdominal distension and bilious vomiting persisted.Histopathological examination of all specimens revealed immature ganglion cells with no hypertrophic nerve bundles(Fig. 3a). Conservative treatment like frequent rectal wash, NG drainage, I/V fluids and prokinetics failed to improve his condition. Therefore, re-laparotomy was performed at 9 days of life. Operative findings were similar to previous laparotomy findings. Resection of the isolated jejunal segment with end to end jejuno-ileal anastomosis and loop ileostomy were performed. Post-operative period was uneventful and patient was discharged on 6th post-operative day. Histopathological examination of the resected dilated jejunal segment showed normal morphology with mature ganglion cells, subserosal neutrophilic suppuration was presentwhile muscularis propria and mucosa were normal (Fig. 3b). Immunohistochemistry was not performed due to financial constraint. Patient is now 1 month old and awaiting ileostomy closure.
Discussion
Congenital Segmental Intestinal Dilatation(CSID) is a rare condition defined as limited bowel dilatation with a three to four fold increase in size with an abrupt transition between the normal and dilated bowel and no intrinsic or extrinsic barrier distal to the dilatation. It was first described by Swenson and Rathauser, and over 150 cases have been reported since then, but none of them provide any clues to the definite etiology of this disease.[2] In the neonatal period, it may present with acute intestinal obstruction or can mimic volvulus or Hirschsprung disease. [6] In older infants, it presents with anemia, malabsorption, chronic constipation, features of intussusception, or intermittent intestinal obstruction.[7] Rathauser in 1959 established the criteria for the diagnosis of this rare entity
[8] which included (i) limited bowel dilatation with a 3-fold to 4-fold increase in size, (ii) an abrupt transition between dilated and normal bowel, (iii) no intrinsic or extrinsic barrier distal to the dilatation, (iv) clinical picture of intestinal occlusion or sub-occlusion, (v) normal neuronal plexus, and (vi) complete recovery after resection of the affected segment.
Segmental dilatation of distal jejunum in this case does fit into all the criteria set by Rathauser [8] except an abrupt transition to normal bowel distally. Therefore, diagnosis of CSID was not made at initial operation and, because of gradual transition to dilated ileum, colonic enteropathy was suspected, hence biopsy was taken from different colonic parts. As this patient’s condition did not improve in the post-operative period, and histopathology of colonic tissues revealed immature ganglion cells, re-laparotomy and resection of the dilated jejunal segment with end to end anastomosis and loop ileostomy were performed considering dubiety of peristalsis of colon.
Histopathological findings of cases described in the literature range from normal findings (just like in this patient) to partial or complete absence of lamina propria in the affected segment to partial hypertrophy of muscle layers with or without an irregular muscular network, minimal thinning of the external muscle layer and degenerated myocytes filled with vacuoles. [2] The presence of ganglion cells was reported in all cases of CSID as part of the criteria. Cheng et al. performed an extended histochemical and immunohistochemical analyses of one instance of jejunal CSID and postulated that segmental dilatation of the small bowel might not originate from the enteric nervous system, but presumed a localized myopathy of the smooth muscle of being at least a part of the source of this entity.[9]
Immature enteric ganglion cells are one form of intestinal neuronal malformation encountered commonly in pre-term and occasionally in term babies.Immaturity of ganglion cells is characterized by the number of ganglion cells either being normal or slightly increased, whereas the nuclear size is small.
[10] It is manifested as transient functional immaturity of large intestine which may sometimes cause intestinal obstruction. Nevertheless, these ganglion cells would mature over time in normal children by the age of 2 to 5 years. Most patients with immature ganglion cells who present with functional obstruction can be treated conservatively with rectal washouts or glycerin suppositories and If conservative management fails, then a stoma should be created. [11], [12]
As it is difficult to quantify the degree of immaturity and the speed at which maturation happens, the exact course of the illness cannot be predicted.
[13] Burki et al,recommend a repeat rectal suction biopsy before stoma closure which should be delayed till 3 months.[4] Alternative approach can be Bishop-Koop distal chimney procedure as a next step to check motility of distal colon, and if functioning properly, final closure can be performed. But, this requires multiple procedures and thereby, increases the risks of morbidity.
In conclusion, CSIPD is a rare intestinal condition, which can be associated with other anomalies like congenital enteric neuropathies. The final diagnosis relies on the intra-operative picture and exclusion of a segmental aganglionosis. Standard therapy is resection of the affected segment and end-to-end anastomosis or using specific surgical procedures depending on the position of the intestinal malformation.
Notes
n1Conflicts of interest. None declared
n3Author contributions: Author(s) declared to fulfill authorship criteria as devised by ICMJE and approved the final version.
n4Consent to Publication: Author(s) declared taking informed written consent for the publication of clinical photographs/material (if any used), from the legal guardian of the patient with an understanding that every effort will be made to conceal the identity of the patient, however it cannot be guaranteed.
References
|
|
| 1. |
Chanchlani R, Seth A, Rakhonde AK. Neonatal gastrointestinal emergencies in a tertiary care center in Bhopal, India: A prospective study. IJSS J Surg. 2015;1:1-4.. |
| 2. |
Brahim MB, Belghith M, Mekki M, Jouini R, Sahnoun L, Maazoun K, et al. Segmental dilatation of the intestine. J Pediatr Surg. 2006;41:1130-3.
. |
| 3. |
Holschneider A, Puri P, Homrighausen LH, Meier-Ruge W. Intestinal neuronal malformation: Clinical expertise and treatment. In:Hirschsprung’s Disease and the Allied Disorders.2008, 3rd ed., pp 232-5.
. |
| 4. |
Burki T, Kiho L, Scheimberg I, Phelps S, Misra D, Ward H, et al. Neonatal functional intestinal obstruction and the presence of severely immature ganglion cells on rectal biopsy: 6 year experience. Pediatr Surg Int. 2011;27:487-90.. |
| 5. |
Takahashi Y, Hamada Y, Taguchi T. Congenital segmental dilatation of the intestine. In: Pediatric Surgery: General Principles and Newborn Surgery, 2020, pp.1099-1105.
. |
| 6. |
Hosie S, Lorenz C, Schaible T, Weber G, Waag KL. Segmental dilatation of the jejunum resembling prenatal volvulus. J Pediatr Surg. 2001;36:927-9.
. |
| 7. |
Mir E, Yegane S, Karaca I, Günşar C, Ceylan H. Segmental dilatation of the jejunum. Acta PaediatrJpn. 1996;38:69-71.
. |
| 8. |
Swenson O, Rathauser F. Segmental dilatation of the colon; a new entity. Am J Surg. 1959;97:734–8.
. |
| 9. |
Cheng W, Lui VC, Chen QM, Tam PK. Enteric nervous system, interstitial cells of Cajal, and smooth muscle vacuolization in segmental dilatation of jejunum. J Pediatr Surg. 2001; 36:930-5.
. |
| 10. |
Taguchi T, Masumoto K, Leiri S, Nakatsuji T, Akiyoshi J. New classification of hypoganglionosis: congenital and acquired hypoganglionosis. J Pediatr Surg. 2006;41:2046–51.
. |
| 11. |
Yamauchi K, Kubota A, Usui N, Yonekura T, Kosumi T, Nogami T, et al. Benign transient non-organic ileus. Eur J Pediatr Surg. 2002; 12:168-174.
. |
| 12. |
Heaton ND, Howard ER, Garrett JR.Small left colon syndrome: an immature enteric plexus. J R Soc Med.1991; 84:113-4.
. |
| 13. |
Kubota A, Imura K, Yagi M, Kawahara H, Mushiake S, Nakayama M, et al. Functional ileus in neonates: Hirschsprung’s disease-allied disorders versus meconium related ileus. Eur J Pediatr Surg.1999; 9:392-5.
. |