Figures

|
|
|
Figure 1
(a) Plain abdominal radiograph showed dilated loops of bowel, (b) microcolon up to hepatic flexure seen on contrast enema. |
|
|
|
|
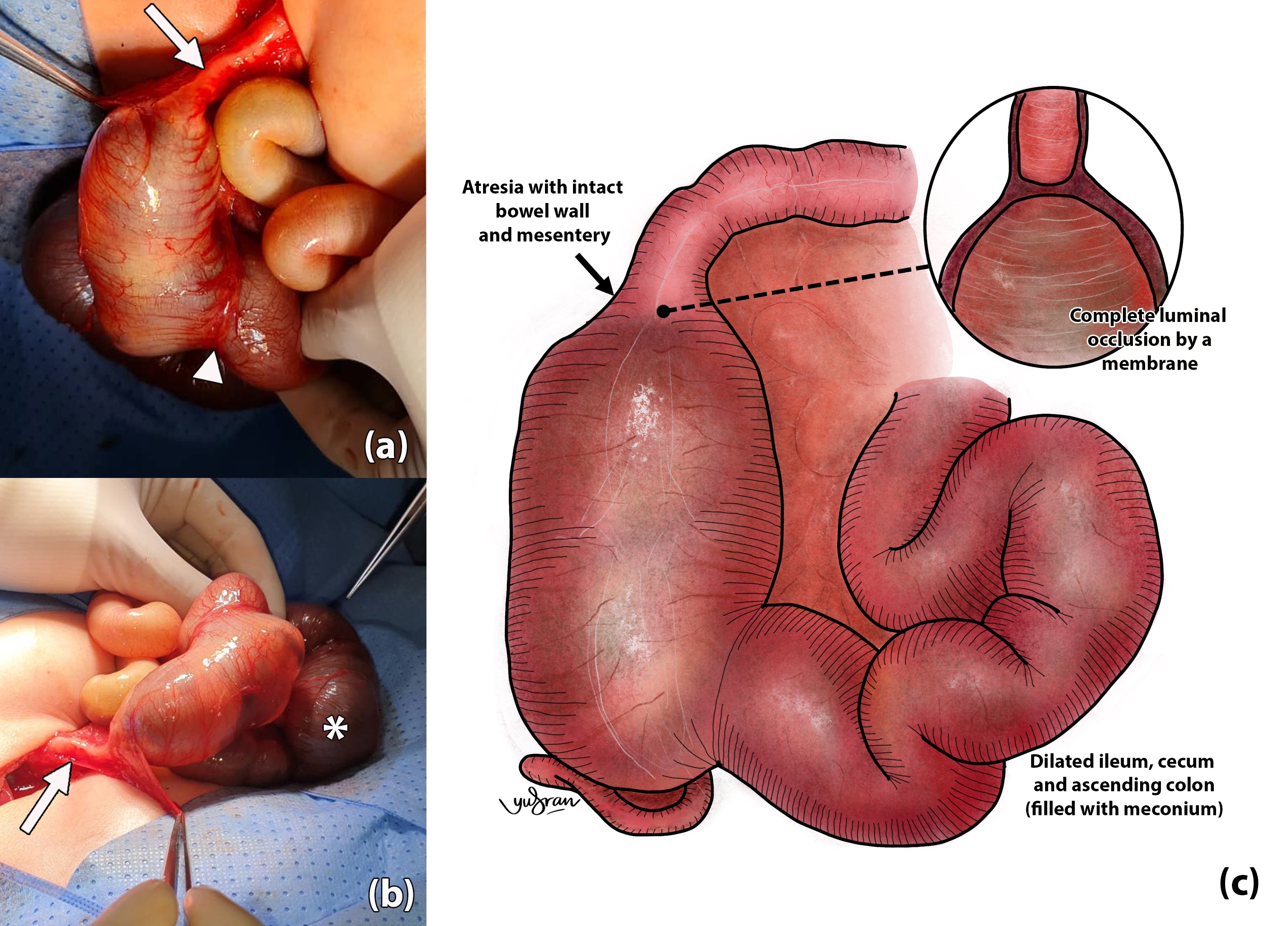
Figure 2
(a, b) Intraoperative findings of colonic atresia at ascending colon with dilated proximal colon and collapsed distal colon (white arrow), wide ileocecal valve (white arrowhead) and dilated distal ileum (white asterisk), (c) illustration to represent the operative findings of type 1 colonic atresia. |
|
Tables
[TableWrap ID: t1]
Table 1
Details of various reported cases of right-sided colonic atresia cases
| Age | Sex | Weight | Site | Type | Primary surgery | Associated anomaly | Outcome | |
| Cox et al.(2005) [3] | - | M | - | Right transverse colon | I | Colostomy | Anorectal agenesis | Survived |
| - | M | - | Right transverse colon | IIIa | Primary anastomosis and covering ileostomy | Two rectal stenosis | Rectal dilatations, Well | |
| - | F | - | Ascending colon | II | Resection, ileostomy | Nil | Survived | |
| Haroon (2010)[12] | 4d | M | - | Ascending colon | I | Colo-colic anastomosis, ileostomy | Nil | Survived |
| Haxhija(2011) [8] | - | M | 4,250g | Hepatic flexure | IIIa | Double-barrel ostomy | Nil | Survived |
| - | F | 3,600g | Hepatic flexure | IIIa | Primary colo-colic anastomosis | Nil | Survived | |
| - | F | 3,260g | Hepatic flexure | IIIa | Double-barrel ostomy | Nil | Survived | |
| - | F | 2,590g | Hepatic flexure | IIIa | Double-barrel ostomy | Volvulus of ileocaecal region | Survived | |
| - | M | 3,370g | Ascending colon | IIIa | Double-barrel ostomy | Gastroschisis | Survived | |
| - | M | 3,000g | Caecum | IIIa | End ileostomy | Gastroschisis | Survived | |
| - | F | 1,600g | Ascending colon | IIIa | End-jejunostomy and colostomy | Gastroschisis & volvulus | Died | |
| - | M | 2,780g | Hepatic flexure | IV | End-to-end colostomy | High jejunal atresia | Survived | |
| - | M | 3,380g | Ascending colon | IV | End-ileostomy | High jejunal atresia | Survived | |
| Bilal Mirza (2013) [11] | 2d | M | 2,500g | Ascending colon | I | Colocolic anastomosis and covering ileostomy | Nil | Survived |
| 1d | F | 2,700g | Ascending colon | I | Colocolic anastomosis and covering ileostomy | Nil | Survived | |
| 3d | F | 2,800g | Ascending colon | III | Colocolic anastomosis and covering ileostomy | Nil | Survived | |
| 1d | M | 2,200g | Ascending colon | I | Colo-colic anastomosis with covering ileostomy, pyloroduodenal anastomosis | Pyloric atresia | Succumbed to sepsis | |
| 3d | F | 2,900g | Hepatic flexure | III | Colocolic anastomosis and covering ileostomy | Nil | Survived | |
| 2d | M | 2,500g | Hepatic flexure | III | Double-barrel ostomy | Nil | Survived | |
| Gobran(2013)[5] | 1d | M | - | Ascending colon | II | Colocolic anastomosis | Nil | Anastomotic dysfunction, survived |
| 1d | M | - | Ascending colon | III | Ileocolic anastomosis | Nil | Survived | |
| 1d | F | - | Ascending colon and hepatic flexure | III | Colocolic anastomosis | Unilateral cleft lip | Survived | |
| 1d | M | - | Ileocecal | III | Ileocolic anastomosis | Ileal atresia | Survived | |
| 5d | M | - | Ascending colon | I | Ileocolic anastomosis | Nil | Survived | |
| El-Asmar et al. (2016)[2] | 2d | F | - | Hepatic flexure | IIIa | Colostomy | Nil | Survived |
| 2d | M | - | Hepatic flexure | II | Primary anastomosis | Type IV small bowel atresia, ASD | Leaking from small bowel anastomosis, sepsis, died | |
| 2m | F | Hepatic flexure | I | Colostomy | Nil | Burst abdomen, survived | ||
| Halder et al. (2017)[7] | 1d | M | 2.6kg | Hepatic flexure | I | Colostomy | Nil | Survived |
| Montenegro (2018)[9] | 3d | F | - | Right colon | III | Hartmann’s colostomy | Nil | Survived |
| Saha (2020)[13] | 4d | M | 2.2kg | Ascending colon | I | Ileocolostomy | Ileal perforation & Meckel diverticulum | Survived |
| 1d | M | 2.5kg | Hepatic flexure | IIIa | Primary resection and anastomosis | Nil | Survived | |
| 4d | M | 2kg | Hepatic flexure | IIIa | Primary resection and anastomosis | Nil | Anastomotic leak, sepsis and died | |
| 2d | M | 1.8kg | Ascending colon | IIIa | Colostomy | Malrotation and ASD | Survived | |
| Tripathy (2020)[6] | 3d | M | 2.1kg | Ascending colon | III | Primary anastomosis and proximal ileostomy | Nil | Sepsis, died |
| 2d | F | 2.1kg | Ascending colon | III | Primary anastomosis, Ladd’s procedure, and abdominal wall defect closure | Gastroschisis | Died | |
| Moaied (2021)[14] | 2d | M | - | Ascending colon | III | Colostomy | Nil | Survived |
| Our case | 1d | M | 3.0kg | Ascending colon | I | Primary anastomosis | Nil | Survived |