Dear Sir
Friemann-Dahl sign is the radiological appearance of three dense lines in the abdomen converging towards the left iliac fossa. It is caused by the apposing walls of the twisted sigmoid colon (sigmoid volvulus). [1] This appearance is also variously known as the ‘omega sign’, ‘bent inner-tube sign’, ‘horse-shoe sign’, ‘convergence sign’, or ‘coffee-bean sign’. Neuhauser’s sign is a soap-bubble like appearance in the right iliac fossa. It is caused by tiny air bubbles entrapped within the viscid meconium of cystic fibrosis. [2] Originally this sign was considered pathognomonic of meconium ileus; but subsequently, it was also reported in necrotizing enterocolitis, Hirschsprung disease, and anal stenosis. [3], [4] Concomitance of both the Friemann-Dahl’s sign and the Neuhauser’s sign in a neonate caused a diagnostic dilemma.
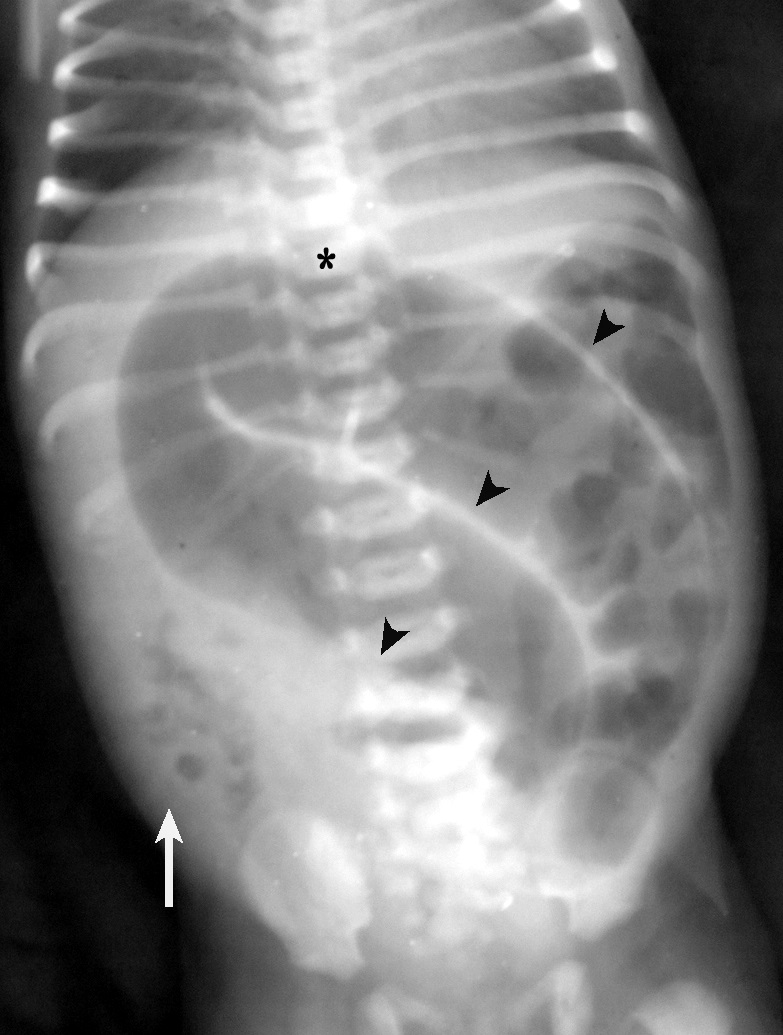
A newborn female was admitted 12 hours after birth with neonatal intestinal obstruction. Physical examination revealed a patent anus. Her abdomen was tensely distended. The plain radiograph showed the typical Friemann-Dahl sign. The apex of the distended bowel loop was at the level of the 8th thoracic vertebral body. Walls of the folded bowel were seen as three opaque lines converging towards the left iliac fossa (Fig. 1). All these features were suggestive of sigmoid volvulus. Scrutiny of the film also showed fine bubbles of gas in the right lower quadrant (Neuhauser’s sign). A contrast enema was not done because of the clinical suspicion of bowel ischemia.
At surgery, the terminal ileum was found to be completely obstructed with inspissated meconium. A loop of the ileum proximal to the site of obstruction was found to be distended and folded, causing the coffee-bean appearance in the plain radiograph. The large bowel was typically that of an unused microcolon. Obstructing meconium could not be kneaded as it was tenacious. Hence, Bishop-Koop ileostomy was performed. Postoperatively, antegrade Gastrografin© lavage was given through the ileostomy to flush out the obstructing meconium. She was discharged on the 16th postoperative day. The ostomy was reversed 3 months later. She is doing fine on a 6-year follow-up. Her workup for cystic fibrosis was negative.
Although rare neonatal sigmoid volvulus is frequently a complication of conditions such as anal stenosis and Hirschsprung’s disease.[5] In contrast, meconium ileus is a common cause of neonatal intestinal obstruction. Features of intestinal obstruction such as abdominal distension, non-passage of meconium, and bilious vomiting are common to meconium ileus, Hirschsprung disease, and sigmoid volvulus. Adding to the diagnostic complexity, meconium ileus, and Hirschsprung disease may precipitate intestinal volvulus. [6]
Hitherto unreported combination of Neuhauser’s sign and Friemann-Dahl’s sign in the same neonate caused a diagnostic dilemma. Conflict resolution in such a scenario involves three principles: [1] As William Osler said, a rare diagnosis will rarely be correct. Although coffee-bean appearance is more eye-catching than the tiny air bubbles of Neuhauser’s sign, the rarity of sigmoid volvulus in neonates deserves due consideration.[2] ‘Multiple fluid levels’ is a characteristic radiographic feature of all intestinal obstructions except meconium ileus. [7] The conspicuous absence of this sign in this neonate adds more credence to the diagnosis of meconium ileus. [3] Decision on further imaging vs surgical exploration should be based on clinical features. In the absence of bowel ischemia, contrast enema would have helped to arrive at the correct preoperative diagnosis. Meconium ileus will show the unused microcolon, while sigmoid volvulus will show the ‘Bird-beak sign’ (also called ‘ace of spade sign’). As the uncomplicated form of both these conditions can also be treated by non-surgical methods, diagnostic enema with water-soluble contrast will also be therapeutic. However, when bowel ischemia is clinically suspected, as it was in our case, contrast enema is contraindicated. Swift laparotomy is essential for both diagnosis and cure.
Notes
n1Conflicts of interest. None
n3Author contributions: Author(s) declared to fulfill authorship criteria as devised by ICMJE and approved the final version. Authorship declaration form, submitted by the author(s), is available with the editorial office.
n4Consent to Publication: Author(s) declared taking informed written consent for the publication of clinical photographs/material (if any used), from the legal guardian of the patient with an understanding that every effort will be made to conceal the identity of the patient, however it cannot be guaranteed.
References
|
|
| 1. |
Stavride E, Plakias C. Coffee bean sign: Its meaning and importance. Clin Case Rep. 2020; 8:2086–7. |
| 2. |
Harris GB, Neuhauser EB, Shwachman H. Roentgenographic spectrum of cystic fibrosis. Postgrad Med. 1963; 34: 251-65. Available from: https://doi.org/10.1080/00325481.1963.11694841. |
| 3. |
Hussain SM, Meradji M, Robben SG, Hop WC. Plain film diagnosis in meconium plug syndrome, meconium ileus and neonatal Hirschsprung's disease. A scoring system. Pediatr Radiol. 1991; 21:556-9. Available from: https://doi.org/10.1007/BF02012596.
|
| 4. |
Maulik K, Srinivasan S, Saini AG, Saini SS. Soap bubble appearance: an ominous sign. BMJ Case Rep. 2019; 12:e229721. Available from: https://doi.org/10.1136/bcr-2019-229721.
|
| 5. |
Khalayleh H, Koplewitz BZ, Kapuller V, Armon Y, Abu-Leil S, Arbell D. Neonatal sigmoid volvulus. J Pediatr Surg. 2016; 51:1782-5. Available from: https://doi.org/10.1016/j.jpedsurg.2016.06.017.
|
| 6. |
Takacs ZF, Meier CM, Solomayer EF, Gortner L, Meyberg-Solomayer G. Prenatal diagnosis and management of an intestinal volvulus with meconium ileus and peritonitis. Arch Gynecol Obstet. 2014; 290:385-7. Available from: https://doi.org/10.1007/s00404-014-3223-7.
|
| 7. |
White H. Meconium ileus: a new roentgen sign. Radiology. 1956; 66:567-71. Available from: https://doi.org/10.1148/66.4.567.
|