Introduction
Congenital segmental dilatation of intestine is rare with over 150 cases reported so far.[1] The normal intestine abruptly transits to a dilated segment of variable length and diameter (3-4 times) without any evidence of mechanical obstruction.[2] The dilated segment is hypomotile but with normal neuronal connections and ganglion cells. Often, it is a solitary lesion, but multiple sites may be involved.[3] Ileum is the most common site followed by colon, jejunum, and duodenum.[4] The extent may range from a small lesion to as much as near-total colon.[2]
Swenson et al. proposed diagnostic criteria of congenital segmental dilatation of the intestine; and most of the reported cases followed it, except a few.[5] Herein, we report a morphologically different case of congenital segmental dilatation of ileum in a patient with anorectal malformation.
Case Report
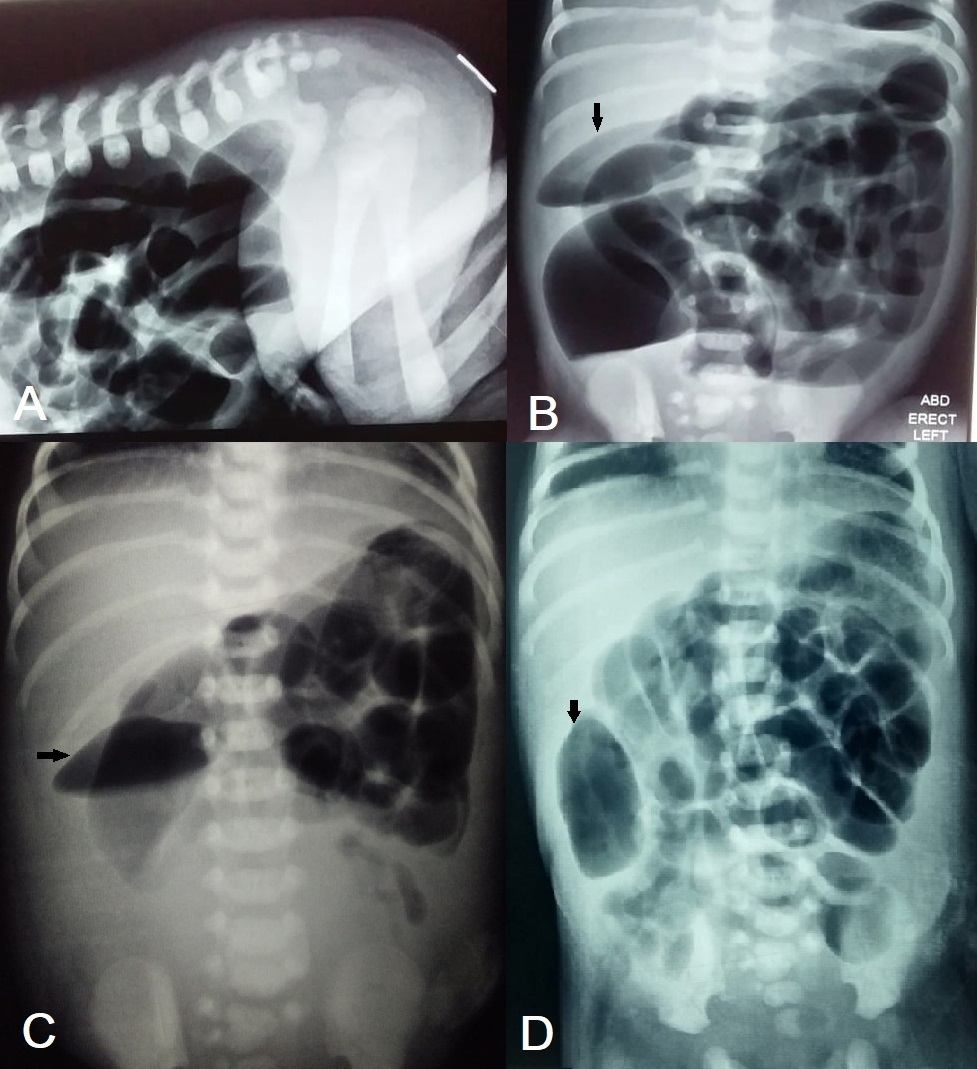
A 1-day-old male neonate, weighing 2.5kg, presented with failure to pass meconium since birth. The baby was born at term by spontaneous vaginal delivery. Antenatal follow-up and perinatal period were uneventful. On examination, the baby had abdominal distension and an imperforated anus. X-ray abdomen (prone cross-table lateral, and erect) showed a high variety of anorectal malformation (Fig. 1A, 1B). Ultrasound of the abdomen revealed normal kidneys. Echocardiography showed a small PDA. The laboratory tests were within normal ranges.
After optimization, the patient underwent sigmoid loop colostomy over a skin bridge as first stage surgery in the management of high variety anorectal malformation. The next day, the patient passed negligible meconium through the stoma. The abdomen further distended and stoma was non-functional.
The repeat X-ray abdomen showed dilated small bowel loops. A fusiform area of bowel gas was noted in the right hemiabdomen that was also present on the initial radiographs. Laboratory tests showed a rising C-reactive protein and declining thrombocytes. The next day, repeated x-rays had the same findings; thus, the parents were counseled for reoperation. A segmental dilated portion of mid-ileum was found at exploratory laparotomy with proximal dilated loops and distal comparatively collapsed bowel(Fig. 2). The abrupt transition from normal bowel to segmental dilatation was absent. The dilated segment was resected, and an ileostomy formed—anastomosis avoided as the baby was getting septic. Serial biopsies were taken from the ileostomy site and colon that excluded Hirschsprung’s disease.
The postoperative recovery remained uneventful. The baby passed adequate stool from ileostomy and was discharged in good condition on ad libitum. The patient is on our follow-up for definitive surgery. We have prioritized ileostomy reversal first, followed by anorectoplasty and colostomy reversal.
Discussion
Congenital segmental dilatation of intestine encounters mostly in neonates (>60%) with a male preponderance.[4] Finding merely case reports and small case series in the literature vindicates its scarcity.[6] Sakaguchi et al. identified 28 cases in a nationwide survey of Japan, over a decade period.[4] We also published a case report in 2012 and a series of 3 cases in 2016.[3], [6]
Two patterns of presentation exist: early with neonatal intestinal obstruction; and late with chronic constipation and related sequelae such as failure to thrive, malnutrition, malabsorption, anemia, etc.[2], [4], [7], [8] Ileal segmental dilatation usually presents early whereas colonic segmental dilatation appears to escape the early presentation, though not a rule.[2], [6], [9]
Associated anomalies may alter the presentation as in the index case; we initially missed the segmental dilatation because the colostomy was formed with a small incision; later we identified it on exploratory laparotomy for persistent intestinal obstruction. We have reported a similar case of imperforate anus with congenital pouch colon where the segmental dilatation was identified on repeat surgery for early postoperative intestinal obstruction.[6]
Antenatal and preoperative diagnoses are seldom, with most cases diagnosed at surgery.[4], [7] Abdominal X-ray, ultrasound, CT scan, and GIT contrast study may help the diagnosis preoperatively; though needs a high index of suspicion. It can mimic other surgical conditions on radiological investigations: pneumoperitoneum on an abdominal radiograph,[6] and duplication cyst on contrast imaging are few examples.[10] In the index case, we initially ignored the discrete fusiform gas shadow on the abdominal radiographs and noticed when the finding persisted on subsequent radiographs.
On literature search, we have identified and classified the varied morphology of the congenital segmental dilatation of the intestine (Table 1). The diagnostic criteria laid by Swensen et al. appear exclusive, but we believe the anomaly has a developmental spectrum, and reported variations in morphology are common.[5], [9] The reported cases differ in site, size, shape, and histology.
Adhikari et al. reported a case of a small congenital segmental dilatation of the jejunum which lacked an abrupt transition between the normal bowel and the segmental dilatation.[5] They initially left it unresected as the mechanical obstruction was absent; on persistent postoperative intestinal obstruction, the lesion was resected at repeat surgery. Such lesions may represent a milder morphological variation (forme fruste) in the spectrum. The index case also appears to be a forme fruste of congenital segmental dilatation of intestine.
Complete surgical resection and anastomosis is curative; however at certain locations (such as the duodenum), tapering is recommended.[4], [7] Occasionally a temporary stoma is needed in cases who are not fit or in sepsis.[9] Similarly in the index case, as the baby was in sepsis, we avoided anastomosis and a stoma was formed.
To conclude, congenital segmental dilatation of the intestine is a rare entity with morphological variations. Rarer still is its forme fruste variant. Occasionally these small lesions are missed on initial surgery thus complicating the treatment course. Complete surgical resection is the treatment of choice in most locations.
Notes
n1Conflicts of interest. MBM and NT are editors of the journal. The manuscript is independently handled by another editor, and they are not involved in the decision making of the manuscript.
n3Author contributions: Author(s) declared to fulfill authorship criteria as devised by ICMJE and approved the final version. Authorship declaration form, submitted by the author(s), is available with the editorial office.
n4Consent to Publication: Author(s) declared taking informed written consent for the publication of clinical photographs/material (if any used), from the legal guardian of the patient with an understanding that every effort will be made to conceal the identity of the patient, however it cannot be guaranteed.
References
|
|
| 1. |
Kasanga TK, Zeng FT, Jampy-Biaya S, Mbuyi AN, Mbuyi-Musanzayi S. Congenital segmental dilatation of the jejunum in an African child: case report. Pan Afr Med J [Internet]. 2021 [cited 2021 Aug 17];38. Available from: https://www.panafrican-med-journal.com/content/article/38/122/full. |
| 2. |
Ragavan M, Arunkumar S, Balaji N. Segmental dilatation of near total colon managed by colon preserving surgery. APSP J Case Rep [Internet]. 2012 [cited 2021 Aug 18];3:18. |
| 3. |
Mirza B, Bux N. Multiple congenital segmental dilatations of colon: a case report. J Neonatal Surg [Internet]. 2012;1:40. Available from: http://www.ncbi.nlm.nih.gov/pubmed/26023399.
|
| 4. |
Sakaguchi T, Hamada Y, Masumoto K, Taguchi T. Segmental dilatation of the intestine: results of a nationwide survey in Japan. Pediatr Surg Int. 2015; 31:1073–6.
|
| 5. |
Adhikari SB, Rana S, Chalise S. Diagnostic dilemma of congenital segmental jejunal pseudo-dilatation associated with immature ganglion cells in the colon: A case report. J Neonatal Surg [Internet]. 2020; 9:13. Available from: https://www.jneonatalsurg.com/ojs/index.php/jns/article/view/jns-532.
|
| 6. |
Rai BK, Mirza B, Hashim I, Saleem M. Varied presentation of congenital segmental dilatation of the intestine in neonates: Report of three cases. J Neonatal Surg [Internet]. 2016 [cited 2021 Aug 17]; 5:55. |
| 7. |
Sergi C, Hager T, Hager J. Congenital segmental intestinal dilatation: A 25-year review with long-term follow-up at the Medical University of Innsbruck, Austria. Am J Perinatol Reports [Internet]. 2019; 09:e218–25. Available from: http://www.thieme-connect.de/DOI/DOI?10.1055/s-0039-1693164.
|
| 8. |
Constanza Janis M, Maricic M, Wurm AL, Medina MS, Díaz SB, Bernatzky A, et al. Segmental dilatation of the intestine. Case report of a typical presentation in a newborn. Arch Argent Pediatr. 2021; 119:E158–62.
|
| 9. |
Nakagawa Y, Harada T, Kaneoka Y. Congenital segmental dilatation of the intestine in extremely low birth weight infants. J Pediatr Surg Case Reports [Internet]. 2020 [cited 2021 Aug 17]; 59:101506. Available from: https://linkinghub.elsevier.com/retrieve/pii/S2213576620301408.
|
| 10. |
Sarin YK, Singh VP. Congenital segmental dilatation of colon. Indian Pediatr. 1995;32:116–8.
|
| 11. |
Khemakhem R, Riazulhaq M, Elhassan EO. Segmental dilatation of intestine presenting as partial intestinal obstruction in a child. APSP J Case Rep. 2014; 5:19.
|
| 12. |
Balik E, Taneli C, Yazici M, Demircan M, Herek. Segmental dilatation of intestine: A case report and review of the literature. Eur J Pediatr Surg. 1993; 3:118–20.
|
| 13. |
Gupta R, Sharma P, Chatterjee A, Shukla AK, Gupta AK, Agrawal LD, et al. Congenital pouch colon with segmental dilatation of ileum: Congenital pouch colon type 6. J Indian Assoc Pediatr Surg [Internet]. 2020 [cited 2021 Aug 19];25(5):319. |